March is National Colorectal Cancer Awareness Month – an ideal time to educate and inform the population about the trends of colorectal cancer (CRC) incidence and mortality in the U.S. New data released by the American Cancer Society predict that of the 153,020 new CRC cases predicted in 2023, 13% (nearly 20,000) will be in individuals younger than 50 years (early-onset CRC). This means improving screening rates in the 45-49 population is even more important. Also important is improving awareness of the signs and symptoms of CRC.
https://coloncancerfoundation.org/wp-content/uploads/2022/09/52241140806_513839e5da_c.jpg421800Emma Edwardshttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngEmma Edwards2023-03-27 11:08:462023-03-27 11:08:46Paying Attention to the Rise in Advanced-Stage Early-Onset CRC
On March 1, 2023, the first day of Colorectal Cancer Awareness Month, the American Cancer Society released some alarming new statistics regarding early-onset colorectal cancer (CRC) diagnoses: in the U.S. population, people are increasingly being diagnosed with CRC at a younger age and with more advanced disease stage. Advanced-stage CRC diagnoses have risen by eight percent in the past two decades. Additionally, early onset diagnoses rose from one in ten individuals in 1995 to one in five in 2019. While CRC in the general population is declining, rates in younger people are on the rise.
The complete report contains CRC incidence, mortality, and screening prevalence data that were derived from multiple national databases, including:
National Cancer Institute
Surveillance, Epidemiology, and End Results (SEER) program
Center for Disease Control
National Program of Cancer Registries
Behavioral Risk Factor Surveillance System
National Center for Health Statistics
National Health Interview Survey
North American Association of Central Cancer Registries
The report projects that of the 153,020 expected CRC cases in 2023, 13% (nearly 20,000) will be in individuals younger than 50. Seven percent of projected CRC mortality will also be in individuals younger than 50. CRC mortality in individuals under the age of 50 is also on the rise, as the mortality rate in this population has risen one percent every year since 2004.
Rising cancer trends in the younger U.S. population point to increased exposures to causal agents, and indicate the need for research that identifies newfound risk factors. The data from this report highlights the growing concern that is early-onset CRC incidence and mortality, pointing to a portion of the population that will need more research and funding in the CRC space.
Efforts to improve screening rates at a health care center in New York City
Racial Disparity in CRC Incidence and Mortality
Racial disparities continue to exist in CRC incidence, mortality, and survival rates. Both incidence and mortality rates in the U.S. are highest among American Indian/Alaskan Native and non-Hispanic Black individuals. Alaskan Native individuals face the highest burden of CRC incidence than any other group (88.5 per 100,000 individuals). Risk factors that contribute to disparities in the Alaskan Native population are likely a combination of environmental factors (low sun exposure, diet low in fiber, smoking, and obesity) and low access to colon health care services. Alaskan Native individuals have the lowest screening rate in the U.S.
Black Americans are more likely to be diagnosed with metastatic CRC than any other racial or ethnic group in the nation. Black patients also experience significant disparities in care, and are 21% less likely to receive colon cancer surgery and 28% less likely to receive rectal cancer surgery. Additionally, Black patients are more likely to develop right-sided tumors, which are correlated with a poorer prognosis.
These updated data from the American Cancer Society point to the need for future research in early-onset incidence, racial disparities, and general risk factors for CRC. Scientists should aim to identify newfound risk factors that are contributing to the trend of CRC diagnoses under 50, and to identify factors specific to high-risk racial and ethnic groups as well.
You can learn more about the signs and symptoms of colorectal cancer on this page.
Emma Edwards is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/08/Screening-e1660914964831.jpg225400Emma Edwardshttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngEmma Edwards2023-03-20 09:20:202023-03-20 09:20:20Colorectal Cancer: New Data Suggest Rising Rates, More Advanced Disease in Young Adults
Biomarkers allow scientists to identify certain diseases from a simple biological sample like urine, breath, or even feces. Volatile organic compounds (VOCs) are the byproducts of metabolic processes associated with cancer, necrosis, or other metabolic changes. Scientists have now identified a new biomarker associated with both colorectal cancer (CRC) and adenoma (noncancerous tumor) that can be used for detection.
The cross-sectional study included 24 newly diagnosed CRC patients, 24 patients with adenomas, and 32 individuals who had a normal colonoscopy between July 2017 and July 2020. Individuals with normal colonoscopies and those with adenomas had fecal samples collected before and after their colonoscopy. Samples were requested from CRC patients 3-4 weeks after diagnosis and before treatment.
Of the 60 VOCs identified, only 3 showed different peaks between CRC and the control groups: p-cresol, 1H-indole, and 3(4H)-DBZ. There was a statistically significant difference between p-cresol peak values in each group with the greatest difference between CRC and the control group. This was also the same for 3(4H)-DBZ. However, 1H-indole did not have a significant difference between the study groups.
After adjusting for sex, age, and body-mass index (BMI), the researchers found that only CRC was associated with increased p-cresol and 3(4H)-DBZ, and p-cresol seemed to be the best possible predictor of CRC. A combination of p-cresol and 3(4H)-DBZ “is also optimistic as a combined biomarker” according to the study authors.
p-cresol was also abundant among patients with adenomas compared to healthy controls. This was also the case after adjusting for age, sex, and BMI.
Although more work needs to be done to determine what processes produce these VOCs, these associations can launch a new set of studies to confirm its use in a clinical setting. Other biomarkers have been identified that can predict CRC occurrence and mortality. Overall, the ability to better detect CRC and precancerous adenomas play an important role in global prevention efforts. A better understanding of the biological processes involved in these diseases is crucial for those efforts to be successful.
Kaylinn Escobar is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2023/03/NCI-on-Unsplash_medical-samples-scaled.jpg25601707Kaylinn Escobarhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngKaylinn Escobar2023-03-08 16:58:272023-03-08 16:58:27 Identifying New Biomarkers in Fecal Samples to Detect Colorectal Cancer
Social media is a powerful tool that can be used to spread important information at unprecedented speed. Many users of TikTok, the short-form video app that has taken the world by storm, have utilized the platform to share their experiences with colonoscopy screenings. Users upload “vlogs” (video blogs) to the platform that document their entire experience in detail and talk to their audience throughout the process. While this may seem like oversharing, the authentic nature of these vlogs has grown popular on TikTok, as videos that do well on the platform often contain genuine and unfiltered content.
One example of this is @lucindabinney‘s three-part video series:
Lucinda Binney walks her audience through her experience with colonoscopy prep in a humorous, unfiltered manner that is popular among many lifestyle influencers. She details her experience with a liquid diet (she includes jello) and the standard practice of taking laxatives to prepare her colon for screening. Through this three-part vlog, she demystifies this screening procedure for her 340,000 followers, coming clean about both her anxiety surrounding the experience and her surprise that the laxative drink didn’t taste as bad as she thought.
While it is uncommon for people in their 20s to receive colonoscopies, as the U.S. Preventive Services Task Force does not recommend them until age 45 (a recent change from the previous age 50 guideline), individuals at high risk for colorectal cancer (CRC) may benefit from receiving a screening. CRC rates in the younger population have risen dramatically in the past two decades, with incidence jumping from 2.7 people per 100,000 in the year 2000 to 5.0 per 100,000 in 2019 in the 15-to-39 age group. While these incidence rates are still not high enough to warrant routine screenings in the general young adult population, they help make the case for increased screenings among those at higher-risk.
Haddon Pantel, MD, of Yale Medicine recommends that people in their 20s and 30s seek CRC screening if they experience any sudden changes in bowel movements, rectal bleeding, or any weight loss, abdominal pain, or appetite changes that are not otherwise explained. For more information about the signs of CRC, check out this resource.
Emma Edwards is a Colon Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2023/02/social-media.jpg9051280Emma Edwardshttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngEmma Edwards2023-02-14 09:00:472023-02-06 12:41:18Impact of Social Media on Colon Cancer Screenings
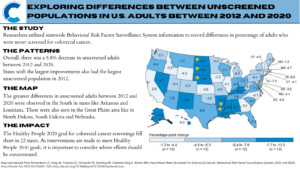
Cancer screening remains a powerful tool. Even limited screening has long-term benefits compared to no screening and can lower the risk of cancer and related deaths. A recent study by researchers at the CDC compared data on adults who reported they had not received a colorectal cancer (CRC) screening test between 2012 and 2020 using information from the Behavioral Risk Factor Surveillance System (BRFSS). The study identified various trends, most notably that 22 states did not meet the CDC’s Healthy People 2020 goal of 70.5% adults screened for CRC.
The sample was limited to adults aged 50 to 75 years, with up to date screenings defined as one of the following:
Home stool-blood test within the past year
Sigmoidoscopy within five years with fecal occult blood test or within one year with fecal immunochemical test
Colonoscopy within ten years
The ‘never screened’ numbers were a composite of those who answered no to being screened or those who were not up to date. Those who declined to answer or reported uncertainty were excluded. Overall, the study identified:
A 5.8% decrease in unscreened adults between 2012 and 2020
States with the largest improvements were also those with the largest unscreened population in 2012
Despite these improvements, CRC screening goals have yet to be met and may be difficult to meet with the new Healthy People 2030 standards. The target of 74.4% screened may have been a challenge to meet, possibly further exacerbated by the COVID-19 pandemic.
Researchers noted that including just two more questions on the BRFSS in 2020, the percentage of up to date screenings increased to 71.6%. These two questions enquired about:
Stool DNA testing
Computerized tomographic colonography
It is important to note that the National Colorectal Cancer Roundtable—a membership organization established by the CDC and the American Cancer Society—has set its goal to 80% screening rates across the country.
Study authors recognized recall bias and an inability to distinguish between screening versus diagnostic tests as major study limitations. Additionally, social desirability bias and a low response rate may have also affected the results. However, financial factors and health disparities may also describe the differences between states.
Following implementation of the Affordable Care Act, researchers at the American Cancer Society found that CRC screening among low-income adults across the U.S. increased by up to 8%, with the greatest increases observed in early Medicaid expansion states. They also noted that a majority of those who were never screened also lived in a state without expansion (South Dakota).
Nonfinancial factors such as health disparities were studied in a mixed-methods analysis conducted at the Virginia Commonwealth University’s School of Medicine. Here, researchers noted that participants of gender-specific and race-specific focus groups brought forth nuanced concerns regarding screening. This included lack of awareness of both the disease and the screening, lack of physician recommendation that is clear and rational, and fear of being diagnosed and complications associated with testing. These concerns, if unaddressed, may limit others from seeking out CRC screening.
To read more about the Healthy People 2030 CRC screening standards and the current progress, visit Healthy People 2030.
Kaylinn Escobar is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/08/Screening-e1660914964831.jpg225400Kaylinn Escobarhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngKaylinn Escobar2023-01-25 08:34:492023-01-25 08:40:06CDC Report: Why Do Certain Populations Never Screen for Colorectal Cancer?
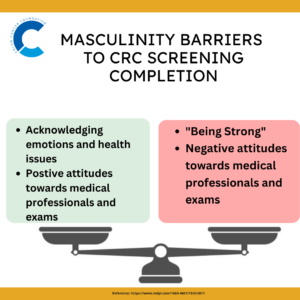
Colorectal cancer (CRC) mortality is preventable with regular screening. Differences in early detection screening rates lead to disparities in CRC mortality among White, Black, and American Indian/Alaska Native (AIAN) men. Complicating the issue of racial disparity observed with CRC screening rates is the psychosocial aspect of men’s health. A recent study investigated the impact of masculinity barriers on CRC screening and found that they influence CRC screening completion.
This survey-based cross-sectional study analyzed the association between the male thought process and the successful completion of CRC screening tests. Male respondents aged 18 to 75 years from across the U.S. who self-identified as Black, AIAN, or white were surveyed. Four Masculinity Barriers to Medical Care subscale were investigated:
Being strong
Acknowledging emotions and health issues
Positive attitude toward medical professionals and exams
Negative attitude toward medical professionals and exams
The highest score, which translates into the greatest barrier for screening, was for “Being strong” and “Negative attitudes towards medical professionals and exams”
Lower scores were observed for “Acknowledging emotions and health issues” and “Positive attitudes toward medical professionals and exams”
For all men, “being strong” was associated with a 54% decreased odds of CRC screening completion.
Reluctancy to seek and engage in preventive health services, such as CRC screening, due to fear of presenting as weak or vulnerable is associated with men who strongly support masculine ideals. The investigation also demonstrated that Black men who scored higher on negative attitudes toward medical professionals and exams subscale had lower odds of CRC screening uptake. The sensitivity analysis of the study reflected that AIAN men had lower odds of CRC completion than Black men.
Medical mistrust is positively correlated with masculine ideologies. Despite decreasing CRC incidence and mortality rates in adults ages 50 years and older, early-onset CRC has increased among adults younger than 50 and is predicted to increase by 90% by 2030. Considering the above masculinity barriers in future population-based and intervention research is critical for increasing men’s participation in CRC screening.
Sahar Alam is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/12/Man.jpg534800Sahar Alamhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngSahar Alam2022-12-22 08:37:482022-12-22 09:03:55Masculinity May be a Barrier to Completing Colorectal Cancer Screening
Initiating regular screening at the recommended age and time interval is key to preventing and early diagnosis of colorectal cancer (CRC). An early CRC diagnosis improves survival. The American Cancer Society (2018) and the U.S. Preventive Services Task Force (2020) recommended that CRC screening should start at 45 instead of 50 years, in reaction to the growing incidence of CRC among younger people.
All major U.S. guidelines now endorse average-risk CRC screening at 45 years of age. However, there are concerns that endoscopic capacity may be strained, that low-risk persons may self-select for screening, and that calculations of the adenoma detection rate may be diluted.
A new study supports the recommendation that colonoscopies should start at age 45, not 50 years. In this study, researchers compared colonoscopy volumes and lesion detection rates in the U.S. healthcare system before (October 2017 to December 2018) and after (January 2019 to August 2021) the new guidelines were issued. They included 7,990 patients who had undergone colonoscopies from October 2017 through August 2021: 4,266 first-time colonoscopies and 3,724 re-screening colonoscopies.
Researchers found that:
After the screening age for colonoscopy was lowered, younger people were more likely to undergo the procedure
Among people ages 45 to 49, first-time screening rates increased from 3.5% in the period before guidelines were changed to 11.6% after they were updated
First-time colonoscopies were still largely performed in patients ages 50 to 54 in both time periods, while re-screening colonoscopies showed a shifting trend toward older ages
Patients ages 60 to 64 were the most likely to undergo re-screening during both time periods
They concluded that in our healthcare system in the early contemporary era of updated CRC screening guidelines, screening colonoscopy volume among 45- to 49-year-old patients has increased modestly, and lesion detection rates in 45- to 49-year-old patients have not decreased as might have been seen if low-risk persons were self-selecting for screening. The authors acknowledged that their findings were based on a single healthcare system and that national data will be important to assess the impact of the revised guidelines.
Kitty Chiu is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/08/Screening-e1660914964831.jpg225400Kitty Chiuhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngKitty Chiu2022-12-13 09:01:552022-12-09 15:02:54Have Colonoscopy Rates Among 45-49 Year Olds Improved After Guideline Change?
Genetic factors play an important role in the development of colorectal cancer (CRC). Some people have inherited genetic syndromes that increase their risk for colon cancer. Genetic testing looks for these inherited syndromes along with changes in DNA that are associated with a greater likelihood of developing cancer.
What is Genetic Testing for CRC?
Genetic testing looks for changes in your DNA that are known to be associated with an increased risk of cancer. Generally, there are two ways that genetic testing may be used:
Before a person develops cancer to determine their level of risk
Following a cancer diagnosis to see if genetic changes may have contributed to the cancer
According to the American Cancer Society, genetic tests can help show if members of certain families have inherited a high risk of CRC due to inherited cancer syndromes such as Lynch syndrome (also known as hereditary non-polyposis colorectal cancer, or HNPCC) or familial adenomatous polyposis (FAP).
Who is Considered “High-Risk”?
Those with a family history of CRC may benefit from speaking to their primary care physician, oncologist, or surgeon about the importance of genetic testing to identify if there was a mutated gene that predisposes them to cancer. You may be a good candidate for genetic testing for CRC if you have:
Close family members, such as parents, children, or siblings, who have been diagnosed with CRC
Many people on one side of your family who’ve been diagnosed with CRC
A personal or family history of CRC diagnosis at a young age
A personal or family history of an inherited genetic syndrome that increases CRC risk
A personal or family history of multiple cancers
A strong family history of CRC or other cancers that are associated with an inherited genetic syndrome
More than 10 adenomatous polyps found during CRC screening
What Can I Expect With the Procedure?
If your doctor believes that you’re a good candidate for genetic testing, they’ll likely refer you to a genetic counselor. Genetic testing is typically done using a blood sample. However, it may also use a sample of saliva, cheek cells, or skin. This sample will be sent to a specialized lab that will run the test. After a few weeks, your results will be sent over to your doctor or genetic counselor and you’ll be contacted to discuss your test results and next steps.
How Much Does Genetic Testing for Colon Cancer Cost and is it Covered by Insurance?
Genetic testing can be expensive and can cost between $100 to over $2,000, depending on the nature and complexity of the test. Many insurance providers will cover the cost of genetic testing and genetic counseling if it’s considered medically necessary.
Most private health insurers cover genetic counseling and testing with low- or no out-of-pocket costs for people who meet certain personal or family cancer history criteria.
Medicare covers genetic testing for people with a cancer diagnosis who meet certain criteria; you must have a cancer diagnosis to qualify for coverage of genetic testing for an inherited mutation.
Medicaid programs cover BRCA genetic counseling and testing for qualifying individuals, including those with a known mutation in the family, or specific personal and/or family history of cancer for all but two states: Alabama and Rhode Island.
Nevertheless, always check with your insurance provider to see what’s covered before getting tested. For additional information about insurance coverage, please visit: Paying for Genetic Services.
Kitty Chiu is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/09/DNA_genetic-testing.jpg225400Kitty Chiuhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngKitty Chiu2022-11-29 08:57:422022-11-29 08:57:42What Do I Need to Know About Genetic Testing for Colorectal Cancer?
As we emerge from the initial waves of COVID-19, patients may have been reluctant to take more time out of their life for a colonoscopy prep, procedure, and recovery. Fortunately, non-invasive stool-based screening tools, such as fecal immunochemical tests (FIT) and multi-target stool DNA (mt-sDNA or Cologuard), are practical options that allow patients to provide a sample in the comfort of their home and could address access and care gap issues as they are less expensive.
According to a new study presented during the Scientific Forum at the American College of Surgeons Clinical Congress 2022, these non-invasive stool-based screening methods are equally effective for screening for early-stage colorectal cancer (CRC). Pavan K. Rao, MD, a general surgery resident at Allegheny Health Network in Pittsburgh, Pennsylvania, presented study results that evaluated 117,519 enrollees within the Highmark claims database who underwent CRC screening in 2019. The researchers found:
About 60% of patients taking either the fecal immunochemical test or the DNA test at home instead of having a routine colonoscopy had early-stage cancer, but a FIT detected it at one-fifth the cost.
The total annual costs for the tests were $6.47 million—$1.1 million for a FIT (about $24 per test) and $5.6 million for mt-sDNA (about $121 per test). Costs were calculated using Medicare reimbursement rates.
Transitioning all non-invasive CRC screening to FIT would result in $3.9 million in savings annually in the study population.
Similarly, these results support previous studies out of Japan and the Netherlands that found FIT was more cost-effective than other types of non-invasive CRC screening tests. This provides our healthcare system with an efficient alternative at a reduced cost that maintains patient outcomes without compromising the quality of care.
https://coloncancerfoundation.org/wp-content/uploads/2022/11/cost_money.jpg600800Kitty Chiuhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngKitty Chiu2022-11-05 15:50:152022-11-05 15:50:15Fecal Immunochemical Tests Affordable and Effective for Colorectal Cancer Screening
Colorectal cancer (CRC) screening is a vital preventative method to detect and remove a polyp and to diagnose cancer before it advances to an incurable stage. CRC screening options include endoscopy and stool-based testing. Now a new study that surveyed unscreened individuals at average risk for CRC has found that people have a preference for the stool-based screening option.
The third most diagnosed cancer in the U.S., over 5 million people worldwide currently live with CRC. One method of CRC screening is a colonoscopy, which detects swollen, abnormal tissues, polyps, or cancer in the large intestine (colon) and rectum. Another form of CRC screening is the fecal immunochemical test (FIT). FIT is one of the most widely used CRC screening methods globally and is an affordable screening tool for studying large populations. FIT detects hidden blood in stool, a potential early sign of cancer, and it has an overall 95% diagnostic accuracy for CRC.
It is estimated that 106,180 new colon cancer cases and 44,850 new rectal cancer cases will be diagnosed in the U.S. in 2022. With the screening age for CRC for average-risk adults lowered to 45 years, we need a better understanding of what the various age groups may prefer as a screening option to improve compliance and screening rates.
The new study that was published has found that individuals in the 40-49 age group and those ≥50 years prioritized test modality above effectiveness when choosing their screening test. The findings of this study demonstrate that:
Both 40-49-years-old and ≥50-year-old age groups preferred FIT-fecal DNA every three years
The second preferred test for both age groups was a colon video capsule, or capsule endoscopy, every five years
Regarding only the USPSTF tier 1 tests, both age groups preferred an annual FIT over a colonoscopy every ten years
68.9% of 40-49-year-olds and 77.4% of ≥50-year-old participants preferred an annual FIT
These results conflict with current CRC screening approaches in the U.S., where colonoscopy is the screening test customarily used. Furthermore, these findings prompt the modification of current CRC screening guidelines and suggest that healthcare providers consider sequential-based screening procedures where FIT is offered before colonoscopy. The results, however, are consistent with a 2007 study, which supports the effectiveness of providing FIT before colonoscopy—the percentage of patients that were up-to-date with screening increased by almost 50% between 2000 and 2015 when they were offered direct-to-patient annual FIT outreach with colonoscopy.
Scheduling delays and longer waiting times for colonoscopies have increased as millions of newly eligible individuals need a colonoscopy, all of which can strain resources and delay access and early screening for patients, especially for those at greater risk for CRC. Sequential approaches for CRC screening, such as those that offer FIT before colonoscopy, can help acknowledge and adjust to the increased need for screening and the lack of resources and help prioritize access to colonoscopy for those at greater risk for CRC.
Sahar Alam is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.
https://coloncancerfoundation.org/wp-content/uploads/2022/10/DNA-in-a-test-tube.jpg450800Sahar Alamhttps://coloncancerfoundation.org/wp-content/uploads/2017/01/CCCF_Logo_Final_Color.pngSahar Alam2022-11-01 08:40:072022-11-01 08:40:07Patient Preference Key to Success of Colorectal Cancer Screening Programs