On March 1, 2023, the first day of Colorectal Cancer Awareness Month, the American Cancer Society released some alarming new statistics regarding early-onset colorectal cancer (CRC) diagnoses: in the U.S. population, people are increasingly being diagnosed with CRC at a younger age and with more advanced disease stage. Advanced-stage CRC diagnoses have risen by eight percent in the past two decades. Additionally, early onset diagnoses rose from one in ten individuals in 1995 to one in five in 2019. While CRC in the general population is declining, rates in younger people are on the rise.
The complete report contains CRC incidence, mortality, and screening prevalence data that were derived from multiple national databases, including:
- National Cancer Institute
- Surveillance, Epidemiology, and End Results (SEER) program
- Center for Disease Control
- National Program of Cancer Registries
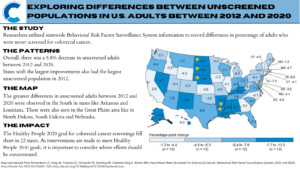
- Behavioral Risk Factor Surveillance System
- National Center for Health Statistics
- National Health Interview Survey
- North American Association of Central Cancer Registries
The report projects that of the 153,020 expected CRC cases in 2023, 13% (nearly 20,000) will be in individuals younger than 50. Seven percent of projected CRC mortality will also be in individuals younger than 50. CRC mortality in individuals under the age of 50 is also on the rise, as the mortality rate in this population has risen one percent every year since 2004.
Rising cancer trends in the younger U.S. population point to increased exposures to causal agents, and indicate the need for research that identifies newfound risk factors. The data from this report highlights the growing concern that is early-onset CRC incidence and mortality, pointing to a portion of the population that will need more research and funding in the CRC space.
Efforts to improve screening rates at a health care center in New York City
Racial Disparity in CRC Incidence and Mortality
Racial disparities continue to exist in CRC incidence, mortality, and survival rates. Both incidence and mortality rates in the U.S. are highest among American Indian/Alaskan Native and non-Hispanic Black individuals. Alaskan Native individuals face the highest burden of CRC incidence than any other group (88.5 per 100,000 individuals). Risk factors that contribute to disparities in the Alaskan Native population are likely a combination of environmental factors (low sun exposure, diet low in fiber, smoking, and obesity) and low access to colon health care services. Alaskan Native individuals have the lowest screening rate in the U.S.
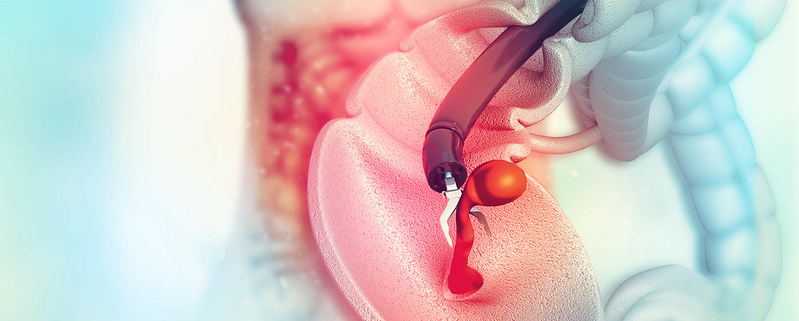
Black Americans are more likely to be diagnosed with metastatic CRC than any other racial or ethnic group in the nation. Black patients also experience significant disparities in care, and are 21% less likely to receive colon cancer surgery and 28% less likely to receive rectal cancer surgery. Additionally, Black patients are more likely to develop right-sided tumors, which are correlated with a poorer prognosis.
These updated data from the American Cancer Society point to the need for future research in early-onset incidence, racial disparities, and general risk factors for CRC. Scientists should aim to identify newfound risk factors that are contributing to the trend of CRC diagnoses under 50, and to identify factors specific to high-risk racial and ethnic groups as well.
You can learn more about the signs and symptoms of colorectal cancer on this page.
Emma Edwards is a Colorectal Cancer Prevention Intern with the Colon Cancer Foundation.